Author: Dr. Bhupendra Gaidhane, Plastic Surgery | Diamond One Building, Dhantoli, Nagpur
Quick Answer
Chest fat (pseudogynecomastia) is caused primarily by excess body fat, while gynecomastia involves enlargement of glandular breast tissue beneath the nipple. Chest fat often improves with weight loss and exercise, whereas true gynecomastia usually persists despite fitness efforts and may require surgical treatment if gland tissue is present.
It usually doesn’t start with a diagnosis.
It starts with a loose T-shirt.
Then comes the habit of standing slightly turned away in photos. Skipping swimming. Choosing darker colours. Avoiding fitted clothes you’d otherwise wear.
For most men who come to consult at my clinic in Nagpur, the chest concern started somewhere in their teenage years. They noticed a fullness, a puffiness under the nipple, or a slight projection when they looked sideways in the mirror. Some were told it would go away. Some started working out harder. Some waited years.
But the chest didn’t change.
That’s when the question becomes very real: is this chest fat — or is it gynecomastia?
Because the answer changes everything about how it should be addressed.
Key Takeaways
- Chest fat is soft and usually associated with overall weight gain.
- Gynecomastia contains firm gland tissue beneath the nipple.
- Weight loss can improve chest fat but cannot remove gland tissue.
- Puffy nipples are more commonly associated with gynecomastia.
- Many patients have a combination of fat and gland tissue.
- A clinical examination is the most reliable way to distinguish between the two.
Why This Confusion Is So Common
From the outside, chest fat and gynecomastia can look nearly identical. Both cause fullness in the chest. Both can create a soft, rounded appearance. And neither responds well to shame or wishful thinking.
But internally, they are completely different:
Chest fat = accumulation of fat tissue in the chest area
Gynecomastia = enlargement of the male breast gland tissue itself
This distinction matters because fat responds to diet, exercise, and liposuction. Gland tissue does not respond to diet or exercise — it requires surgical excision to be removed. Treating one when the patient has the other leads to incomplete results and frustration.
Most patients who walk into my clinic after years of gym work and weight loss have not failed. They were simply treating the wrong thing.
What Is Chest Fat (Pseudogynecomastia)?
Chest fat, also called pseudogynecomastia, is the accumulation of fat in the chest area without any gland involvement. It is directly linked to overall body fat and typically appears when fat is deposited unevenly across the torso.
Typical characteristics:
- Soft, compressible feel when pressed
- Diffuse spread across the entire chest — not concentrated under the nipple
- No firm or rubbery lump behind the areola
- Often present alongside fat in the abdomen and flanks
- Improves meaningfully with consistent weight loss
Pseudogynecomastia responds to lifestyle changes and, when needed, liposuction for contouring. There is no gland to remove.
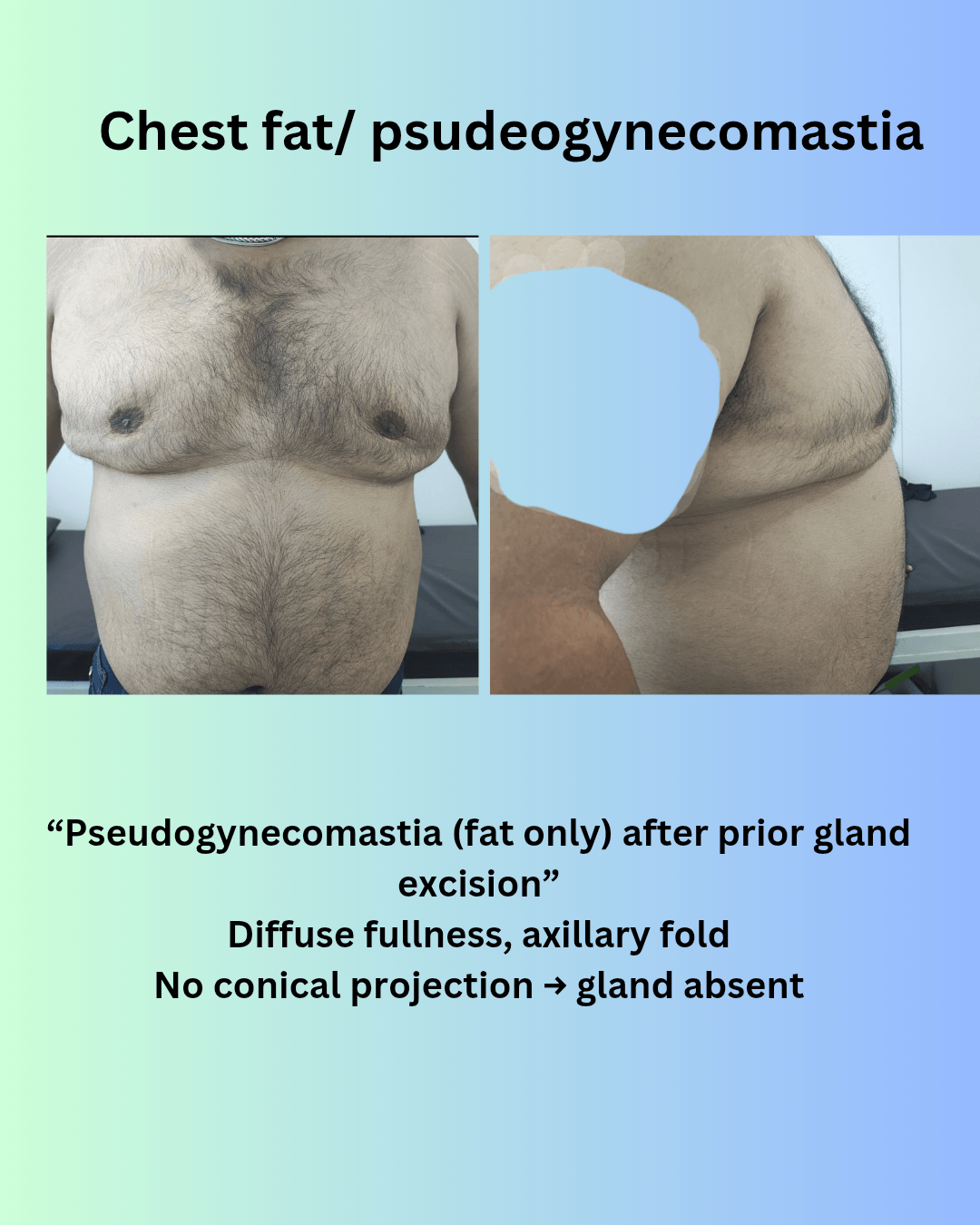
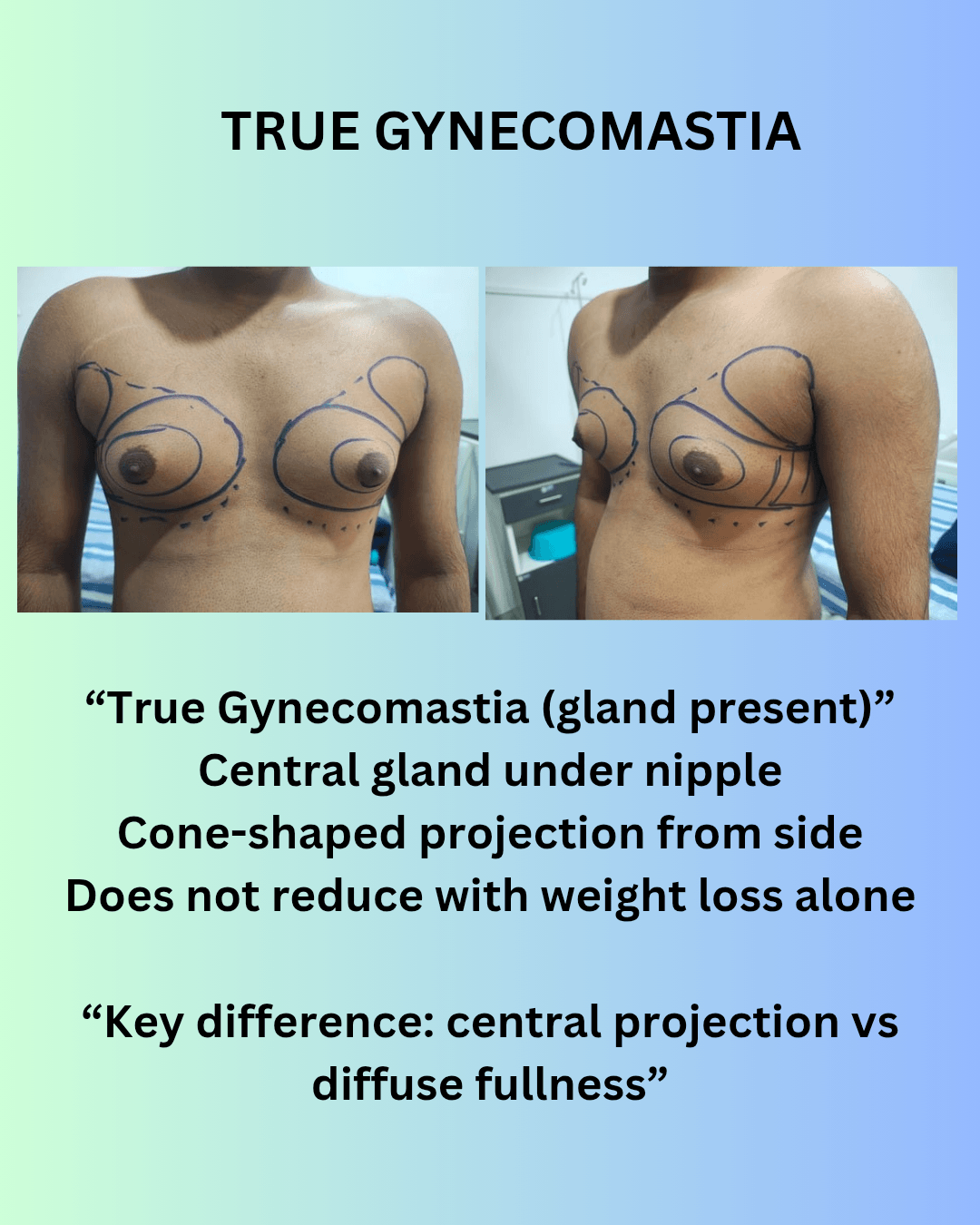
In some patients, chest fullness is due to fat rather than true gynecomastia. This is called pseudogynecomastia. The key difference lies in the presence or absence of gland tissue. Fat deposition tends to be diffuse, spreading across the chest and extending towards the axillary (side) area, often accompanied by overall weight gain. Importantly, there is no firm gland under the nipple and no cone-shaped projection when viewed from the side. In contrast, true gynecomastia involves glandular tissue, which creates a central, firm fullness directly beneath the nipple–areola complex, often giving a characteristic conical or projected appearance. Understanding this difference is essential, because fat may improve with weight loss or liposuction, whereas glandular gynecomastia does not resolve with exercise alone and typically requires surgical excision.
What Is Gynecomastia?
Gynecomastia is the enlargement of glandular tissue in the male breast. It often begins during adolescence due to hormonal shifts, and in many men it does not fully resolve on its own. It can also develop in adulthood due to medications, hormonal imbalances, or other causes.
Typical characteristics:
- A firm or rubbery disc of tissue felt directly under the nipple
- Puffy or enlarged areola
- A cone-shaped projection visible from the side profile
- Present even in lean individuals
- Does not reduce significantly with exercise or weight loss
Gynecomastia is not a fat problem. It is a gland problem. No amount of gym work removes gland tissue.
Chest Fat vs Gynecomastia — A Direct Comparison
| Feature | Chest Fat (Pseudogynecomastia) | Gynecomastia |
|---|---|---|
| Feel | Soft, compressible | Firm or rubbery disc |
| Location | Diffuse across chest | Centralised under nipple |
| Shape | Flat or sagging | Cone-shaped projection |
| Effect of weight loss | Reduces noticeably | Usually persists |
| Nipple / areola | Normal appearance | Puffy or enlarged |
| Gym response | Some improvement | No significant change |
| Treatment | Liposuction if needed | Gland excision + liposuction |
How to Do a Self-Examination at Home
Many men search for ways to assess themselves before deciding to consult. Here is a practical approach that gives useful preliminary information — though it is not a substitute for clinical assessment.
Step 1 — Mirror check
Stand in front of a mirror in good light. Look at your chest from the front, then turn sideways. Note whether there is a cone-shaped projection from the side, and whether the nipple or areola appears puffy or enlarged compared to the surrounding chest.
Step 2 — The pinch test
Using your thumb and index finger, gently compress the tissue behind the nipple. Soft, pliable tissue that compresses evenly suggests fat. A firm, disc-like structure that resists compression and feels distinctly different from the surrounding tissue suggests gland.
Step 3 — The flex test
Tighten your chest muscles as if posing. Fat tissue tends to blend and flatten with the muscle underneath. Gland tissue tends to remain prominent and unchanged — it sits on top of the muscle and does not respond to flexion.
Step 4 — Symmetry check
Fat accumulation tends to be broadly symmetrical across both sides of the chest. Gynecomastia may be uneven — more prominent on one side, or with different degrees of gland firmness on each side.
Still unsure? If you can feel a firm disc-like lump directly beneath the nipple that remains despite weight loss, true gynecomastia is more likely than simple chest fat.
What self-examination can and cannot tell you
Self-examination helps you understand whether your concern is more likely fat, gland, or a mixture of both. It cannot determine the grade of gynecomastia, the ratio of fat to gland, or what treatment is appropriate. The majority of men presenting for evaluation have a combination of both — and that combination requires clinical assessment to quantify accurately.
How Gynecomastia Is Assessed During a Clinical Consultation
This is where a preliminary idea becomes a clear diagnosis and a structured plan.
Visual assessment — front and side view
The chest is examined from both views under consistent lighting. The degree of projection, the areolar size, and the overall chest contour are noted. In more advanced cases, the presence of an inframammary fold — a visible crease below the chest — indicates skin and tissue excess beyond simple gland enlargement.
Muscle contraction test
The patient is asked to flex the chest. This separates fat (which softens and flattens) from gland tissue (which remains firm and visible). It also helps assess how much of the projection is tissue versus skin.
Palpation and layer analysis
This is the most informative part of the examination. Each layer is individually assessed:
- The fat layer — depth and distribution across the chest and into the lateral chest and axillary area
- The gland — size, firmness, position relative to the nipple, and extent
- The skin — elasticity and likelihood of adequate retraction after tissue removal
Axillary fullness
In some patients, tissue extends toward the armpit — what is often called the axillary roll or lateral chest fullness.
Grade assessment
Gynecomastia is typically graded from Grade I to Grade IV. The grade determines the surgical approach.
Why Gym Alone Does Not Solve This
This is one of the most common frustrations I hear:
“I have been working out for two years. My body has changed everywhere. But the chest looks the same.”
There is a straightforward reason for this. Exercise reduces body fat, including chest fat. But it has no effect on gland tissue. If a patient has even a moderate gland component, the chest will continue to project regardless of how lean or muscular they become. In some cases, as the surrounding fat reduces and the muscle grows, the gland becomes more visible — not less.
This is not a failure of effort. It is a misunderstanding of what the chest is made of.
Similarly, some patients who previously had gland excision elsewhere report that their chest has “come back.” In most of these cases, what has returned is fat — not gland. True gland recurrence after complete excision is uncommon. Fat deposition, however, continues with weight gain. This is why a combined approach — addressing both fat and gland — gives more stable, natural results over time.
Advanced Signs in Higher Grades
In more advanced presentations, the chest begins to behave more like a breast structurally. Two signs are particularly relevant:
Inframammary fold (IMF)
A visible crease or fold below the chest indicates that the breast mound has developed a defined lower boundary. This suggests tissue and skin excess beyond what liposuction and gland excision alone can address — and requires additional planning for skin management.
Axillary fullness
Tissue extending toward the armpit, sometimes called the bra roll or lateral chest bulge, is more noticeable in fitted clothing and during movement. It needs to be addressed as part of the same procedure for a complete and natural result.
Both signs are common in Grade III and Grade IV cases and require a structured surgical plan rather than a standard approach.
The Role of VASER (Lipovase Technology) in Treatment
In my practice, I use Lipovase — a 4th generation VASER ultrasound-assisted liposuction system — for fat removal in gynecomastia surgery.
Traditional liposuction mechanically disrupts fat. VASER uses ultrasound energy to selectively emulsify fat cells before they are removed, which has specific advantages in gynecomastia treatment:
- More precise fat removal around the gland, reducing the risk of leaving a visible step-off or depression
- Better ability to address the lateral chest and axillary area where tissue transitions are subtle
- Improved skin retraction in many patients due to the effect of ultrasound energy on the subdermal layer
- Smoother overall contour in mixed fat-and-gland cases where the junction between fat and gland needs careful handling
VASER does not replace gland excision — firm gland tissue is still removed through a small periareolar incision. But it substantially improves the quality of fat contouring around the excision, which is what gives the result a natural appearance rather than an operated one.
This technology is particularly useful in mixed cases, higher grades, and patients with lateral chest or axillary involvement.
Treatment Overview
If the concern is primarily chest fat:
- Weight loss and lifestyle changes as first-line management
- Liposuction for contouring if fat persists despite adequate weight loss
- No gland excision required
If it is gynecomastia (gland present):
- Gland excision through a small periareolar incision — this is essential and cannot be replaced by any non-surgical method
- VASER-assisted liposuction for fat contouring around the gland
- Skin management if excess skin is present (more advanced grades)
In most patients — a combined approach:
The majority of men who present for evaluation have both fat and gland in varying proportions. The treatment plan is built around the individual layer analysis — how much fat, how much gland, what grade, and what the skin quality allows. This is why a consultation and clinical assessment is the starting point, not a treatment protocol selected in advance.
Learn more about the procedure in Gynecomastia Surgery in Nagpur
When to Seek an Evaluation
Consider a consultation if any of the following apply:
- Your chest has not improved despite sustained weight loss and exercise
- You can feel a firm or rubbery lump behind the nipple
- The concern has been present since your teenage years
- The chest looks the same or worse as you get leaner
- You notice visible projection from the side profile
- There is asymmetry between the two sides
Why Patients in Nagpur and Surrounding Areas Choose to Consult Here
Patients come from Nagpur, Wardha, Amravati, and other parts of Vidarbha with a common set of concerns: they want a clear diagnosis, an honest assessment of what treatment is appropriate, and realistic expectations about results and recovery.
What I offer at my clinic at Diamond One Building, Dhantoli, Nagpur, is a structured clinical evaluation — not a one-size-fits-all protocol. The layer analysis described in this article is how every patient is assessed. The treatment plan follows from that, not from assumptions.
For patients who require surgery, I use Lipovase (4th generation VASER) for fat contouring and perform gland excision where indicated. Recovery guidance is given clearly before surgery so patients understand the timeline for returning to work, exercise, and normal activity.
Frequently Asked Questions
How do I know if I have gynecomastia or just chest fat?
The most reliable self-assessment is the pinch test — compressing the tissue behind the nipple between your fingers. Soft, uniform tissue that feels the same as the surrounding chest area is more likely fat. A firm, disc-shaped structure that resists compression and sits distinctly under the nipple is more consistent with gland tissue. A side-profile view showing a cone-shaped projection rather than a flat or sagging appearance also suggests glandular involvement. However, most men have a combination of both, and the exact proportion can only be determined through clinical palpation by an experienced surgeon.
Can chest fat turn into gynecomastia?
No. Chest fat and gynecomastia are different types of tissue. Fat does not transform into gland tissue. However, both can coexist in the same patient, which is why the chest may have both a soft component (fat) and a firm component (gland) at the same time.
Will losing weight fix my gynecomastia?
Weight loss can reduce the fat component of chest enlargement, which may improve appearance. It will not reduce the gland component. If gland tissue is present, it will remain after weight loss — and in some lean patients, it becomes more visible as surrounding fat reduces. If your chest has not responded to sustained weight loss and exercise, gland tissue is likely a significant component.
Is self-examination reliable enough to avoid a consultation?
Self-examination gives useful preliminary information and helps you describe your concern accurately. It cannot determine the grade of your condition, the ratio of fat to gland, the quality of your skin, or what treatment approach is appropriate. These require physical examination by a surgeon. If your concern has persisted for more than a year despite lifestyle changes, a consultation is the most efficient next step.
Is surgery always required for gynecomastia?
Not always. Very mild Grade I cases in younger patients with primarily hormonal causes may be monitored. However, once gynecomastia has been present for more than one to two years, the gland tissue becomes fibrous and does not respond to medication or any non-surgical treatment. For established gynecomastia with a firm gland component, surgery is the only method that removes the gland.
What is the recovery like after gynecomastia surgery?
Most patients return to desk work within 3 to 5 days. A compression garment is worn for 4 to 6 weeks. Gym and upper body exercise are typically resumed after 4 to 6 weeks depending on the extent of surgery. The final contour is visible once swelling has fully resolved, which takes approximately 2 to 3 months. Specific recovery instructions are discussed in detail during the pre-surgical consultation.
Many patients face this phase for years before opting for treatment. Read more in Gynecomastia Recovery Timeline
What is VASER liposuction and how is it different in gynecomastia surgery?
VASER uses ultrasound energy to break down fat cells before removal, rather than mechanically disrupting them. In gynecomastia surgery, this allows more precise contouring around the gland, better handling of the lateral chest and axillary area, and a smoother overall result compared to standard liposuction. I use Lipovase, a 4th generation VASER system, for fat management in gynecomastia cases at my clinic in Nagpur.
Can gynecomastia come back after surgery?
Once the gland is completely excised, true gland recurrence is very uncommon. What patients sometimes notice years later is fat deposition — not gland regrowth — especially if there has been significant weight gain. This is why maintaining a stable weight after surgery is important for a lasting result.
I had surgery elsewhere but my chest looks full again. What has happened?
In most cases where this occurs, the fullness is due to fat accumulation rather than gland regrowth. If only the gland was removed previously without adequate fat contouring, or if weight has increased since surgery, the chest can appear full again. A clinical examination is needed to determine whether the fullness is fat, residual gland, or a combination.
At what age can gynecomastia surgery be performed?
Surgery is generally recommended once the hormonal fluctuations of puberty have stabilised, which is typically around 18 years of age. In adults, there is no upper age limit — the assessment is based on the individual’s overall health, tissue characteristics, and realistic expectations rather than age alone.
A Closing Thought
Get Clarity About Your Condition
If your chest has not changed despite years of effort, it is almost certainly not about effort.
The distinction between fat and gland is a clinical one.
If you have been uncertain, a consultation is the most direct way to get clarity.
Consultation available at Diamond One Building, Dhantoli, Nagpur.
Dr. Bhupendra Gaidhane
Plastic & Cosmetic Surgery
Diamond One Building, Dhantoli, Nagpur
This article is written for educational purposes. Clinical assessment is required for diagnosis.
Related Topics
- Gynecomastia Grades Explained
- Gynecomastia Surgery in Nagpur
- Gynecomastia Recovery Timeline
- Liposuction Treatment